Why healthcare customer service doesn't follow the usual AI playbook
When I look at the support queues in most industries - SaaS, ecommerce, fintech - the AI deployment question is mostly about volume and tone. Healthcare is different. Not harder to automate in the abstract, but harder to get wrong. The failure modes have different consequences.
Three things make healthcare support unlike anything else:
Volume with a compliance overlay. Healthcare contact centers receive the same kind of high-repetition, predictable queries that AI handles well in any industry. "Can you reschedule my appointment?" "What's my copay for a specialist?" "I can't log into the patient portal." These are the questions every team fields all day. The difference is that every interaction involving a patient's name alongside their care context is Protected Health Information under HIPAA. That doesn't make it unanswerable by AI - it makes the AI vendor's data-handling posture a procurement prerequisite rather than a nice-to-have.
The administrative vs. clinical line. Other verticals have risk gradations (financial advice vs. account help in fintech, medical device instructions vs. general product info in medtech). Healthcare has a hard wall. Administrative support - hours, billing, scheduling, portal navigation - AI can handle. Clinical support - anything touching symptoms, diagnosis, treatment, or interpretation of results - is a licensed-professional-only zone. Not because the AI couldn't produce a plausible-sounding answer. Because a plausible-sounding clinical answer that's wrong in healthcare is a different category of problem than a wrong answer about shipping timelines.
Accuracy stakes. On Reddit's r/medicine community, one physician put the case for automating the administrative side bluntly: "You know what would be a lot easier to replace with a chatbot? Administrators. Let's do that instead." - u/StepUp_87. The same discussion flagged what makes unscoped AI dangerous: patients already take clinical questions to general-purpose chatbots (ChatGPT, Gemini) that weren't designed for healthcare, don't have clinical guardrails, and have no data-privacy agreement with anyone. A purpose-built, properly scoped AI support agent is a safer outcome than the DIY alternative patients are already using.
What AI can and can't handle in healthcare
The framework I use when talking to healthcare teams is a two-column split. Get this right and the deployment almost designs itself. Get it wrong and you've shipped a tool that sounds confident when it should escalate.
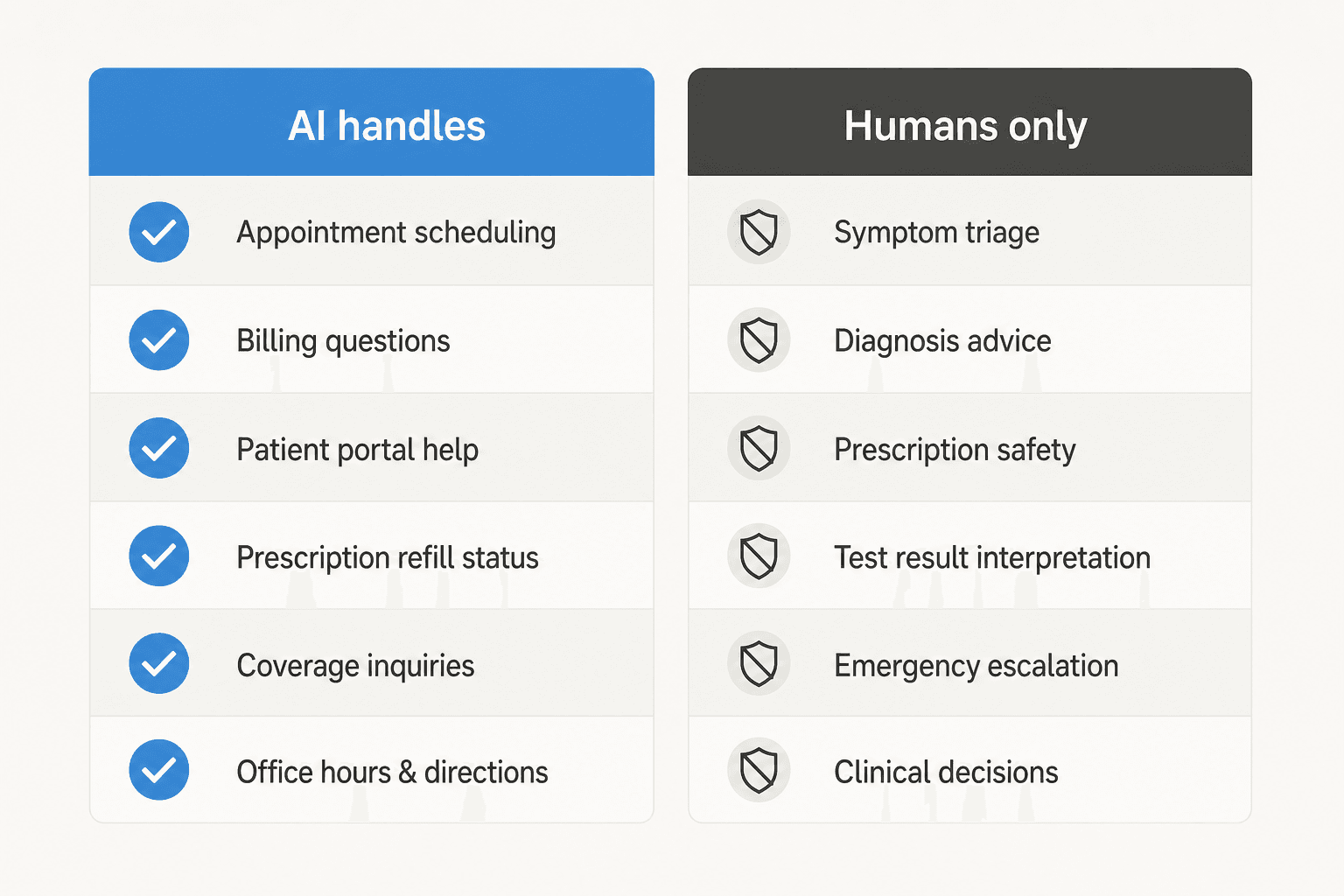
Safe for AI: Appointment scheduling and rescheduling, billing and insurance questions, patient portal help (password resets, navigating records, updating insurance), prescription refill status (not clinical advice - just "is my refill ready?"), benefits and coverage inquiries ("what's my copay for a specialist?"), and general information like office hours, location, and visiting policies.
Humans only: Symptom interpretation and triage, diagnosis or treatment questions, prescription safety questions ("can I take this with my other medication?"), test result interpretation ("my lab results say X, is that normal?"), and anything that requires a licensed clinical judgment.
The cleaner framing: AI answers the question a receptionist could answer. Anything requiring a clinical license routes to a person.
CMS validated the administrative side explicitly in its July 2025 "Make Health Tech Great Again" press release: "Virtual medical assistants may help patients understand their benefits, respond to routine customer inquiries and policy questions, and offer basic claim status updates." That's not a fringe interpretation - the federal government is actively building the infrastructure for AI-assisted administrative patient support, with Amazon, Anthropic, Apple, Google, and OpenAI all committing to patient-facing tools in this category.
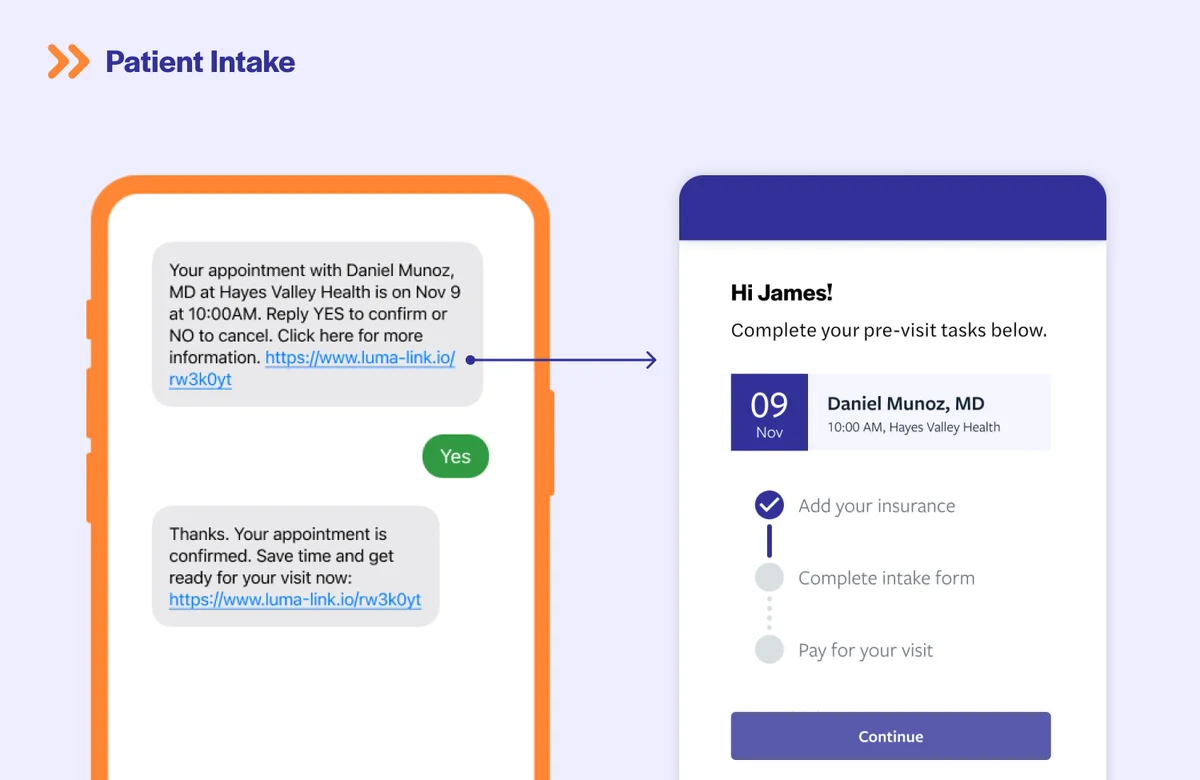
Here's what the split looks like in a real healthcare support context. This is from Luma Health, a patient communication platform that handles the scheduling and intake side:
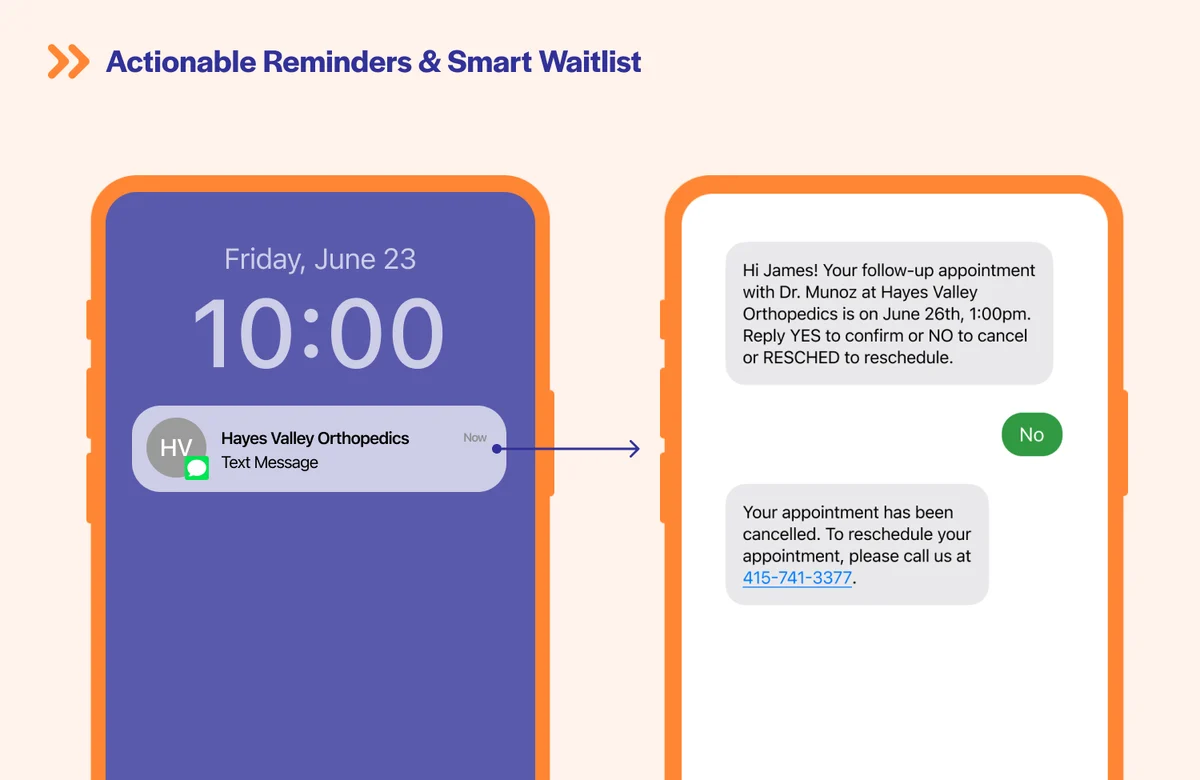
Appointment reminders, rescheduling, and intake prep - all administrative, all AI-appropriate. The system sends the reminder, the patient replies YES or NO, and the slot gets updated. No clinical judgment involved. This is the category that reduces no-shows, frees up staff time, and runs 24/7 without adding headcount.
The patient self-scheduling flow makes the same point:
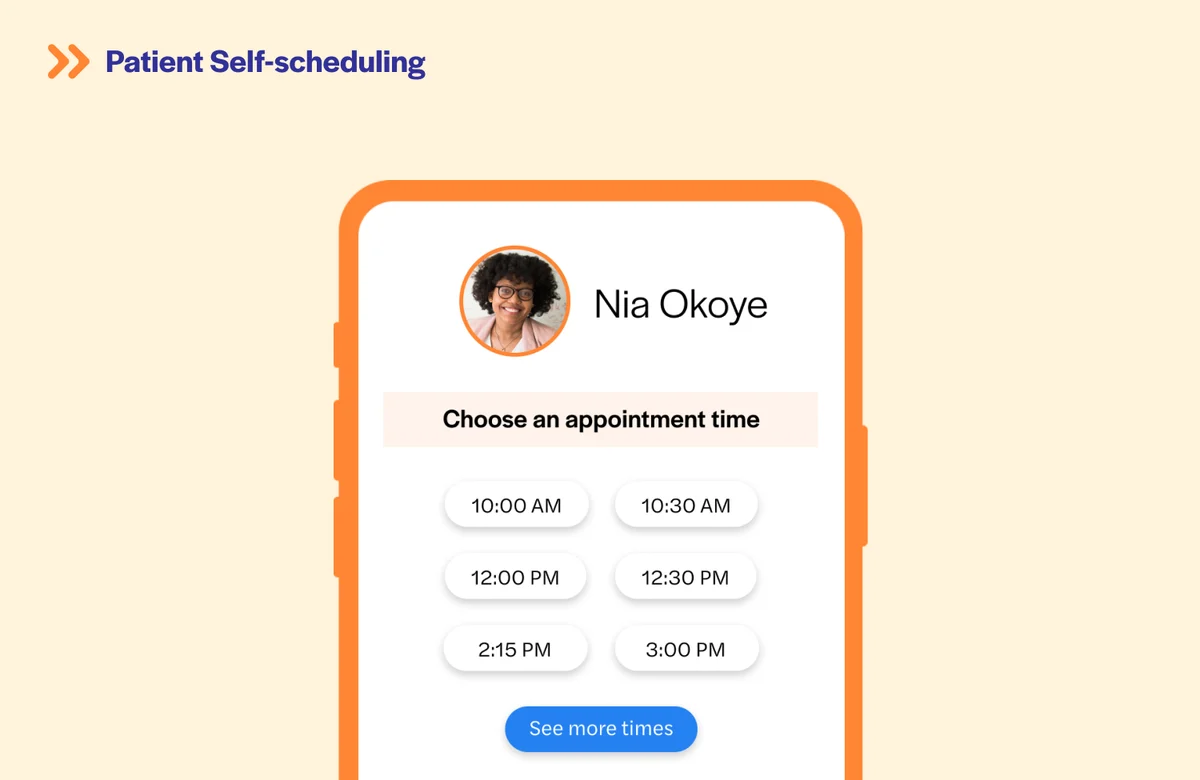
A patient picks a time slot. The AI confirms it. No human involved, no clinical risk - and one fewer call to the front desk. That's agent productivity in practice.
The compliance bar: what to demand before connecting a single ticket
This section decides whether AI customer service actually ships at your healthcare organization. The compliance review is the procurement gate, not the demo.
One practitioner on r/automation put the filter rate plainly in a thread specifically asking about healthcare AI chatbots: "The PHI thing is the real killer - you basically need everything on-prem or in their own cloud environment... Also check if they need BAA agreements.. that usually filters out 90% of vendors right there." - u/expl0rer123 (January 2026).
That's not an exaggeration. Standard tiers of OpenAI, Google, and most consumer AI tools don't offer Business Associate Agreements. You cannot route PHI through them. Full stop.
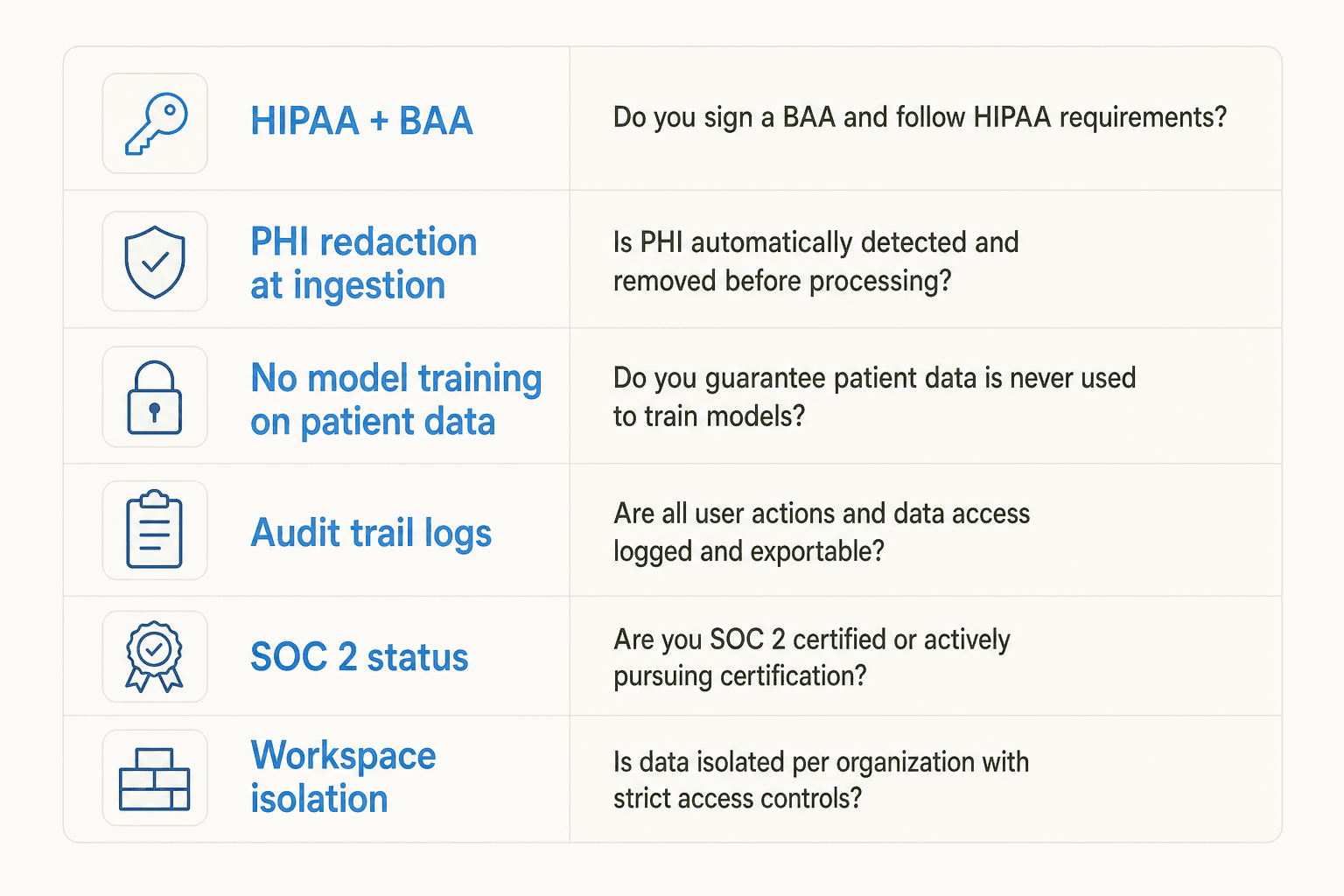
Here's the checklist I'd run on any AI vendor before connecting a healthcare support queue:
| What to demand | Why it matters | The question to ask |
|---|---|---|
| HIPAA + BAA | Any vendor handling PHI must sign one before a ticket flows | "Will you execute a BAA before we start, and is it included in the standard contract or only enterprise?" |
| PHI redaction at ingestion | Patient names, SSNs, insurance IDs, emails in tickets must be stripped before they reach any AI model | "Do you redact PHI at ingestion, and what identifiers does that cover?" |
| No model training on patient data | Your patients' health data cannot go into a shared training corpus | "Is my data ever used to train your models, in any form?" |
| Workspace isolation | No cross-contamination between your data and other customers | "Is my workspace fully isolated from other customers?" |
| Audit logs | HIPAA's Security Rule requires immutable, queryable logs of every AI interaction with ePHI | "What does your audit logging capture, and how long is it retained?" |
| SOC 2 status | The baseline attestation for US data-security procurement | "SOC 2 Type II - certified, in progress, or not started? Can I see the report?" |
| Data deletion | Patient data must be deletable on request | "How do you handle deletion requests, and what's the SLA?" |
The Optum incident from December 2024 is the cautionary tale for what happens when this review gets skipped. UnitedHealth's Optum division left an internal AI chatbot publicly accessible without authentication - used by employees for benefits and operational queries, left exposed to the public internet. The healthcare IT community's reaction was blunt: "Having worked on health insurance tech for 20 years, this is absolutely the expected result of health insurance tech leadership." - u/Prize_Instance_1416. The failure wasn't the AI. It was the deployment without basic access controls. That's the checklist catching the thing the demo doesn't.
Here's where eesel lands on that checklist, because I'd rather show than pitch:
- HIPAA + BAA: Available on the Enterprise plan ($1,000/month flat fee plus usage). Enterprise is the requirement for healthcare teams handling PHI.
- PHI redaction: Strips SSNs, names, emails, phone numbers, card numbers, and API keys at ingestion - before the data reaches eesel's search index or any AI provider. Customer-controlled.
- No model training: "Your data is never included in any training data, period." Standard for all plans.
- Workspace isolation: Each customer's data is fully isolated - no cross-contamination between accounts.
- Audit logs and incident response: Customers notified within 72 hours of any incident. Formal incident-response process with containment and root-cause analysis.
- SOC 2: Type II certification is in progress with Vanta continuous monitoring. Not yet certified - if your procurement team requires the certificate as a non-negotiable today, say so before the contract stage rather than at it.
- Encryption: AES-256 at rest, TLS 1.2+ in transit.
- GDPR + CCPA compliant. EU data residency available on request. Data deletion honored within 60 days.
For the broader AI customer service landscape and which platforms have healthcare-specific certifications, Ada (SOC 2 Type II, GDPR, HIPAA, and PCI DSS certified) is the clearest example of a general-purpose AI customer service platform that has proactively pursued the full enterprise compliance stack. For comparison on how helpdesk platforms handle this, our deep dive on Freshdesk security and SOC 2 is a useful reference point.
Accuracy: the cost of a wrong answer here is different
Most AI customer service failures are recoverable. A wrong shipping estimate gets corrected with an apology and a refund. In healthcare, a wrong answer about medication timing, an incorrectly confirmed procedure coverage, or - worst case - clinical guidance the AI had no business giving can have direct health consequences.
This isn't an argument against AI in healthcare support. It's an argument for gating the AI on confidence.
A clinic dietician and practice manager on G2 described exactly the right instinct when reviewing Tidio for patient communication: "I prefer to reply manually so the communication stays personal for health-related questions." - Ishan S., Chaitanya Homoeo Clinic (February 2026). That's a practitioner who's adopted AI for intake and organization but draws the line at automated patient-facing replies. In a general-purpose helpdesk, that's caution. In a properly scoped deployment, it becomes the starting position: AI drafts, humans approve.
The right AI customer service system in healthcare isn't AI that auto-replies to everything. It's AI that:
- Knows what it knows. Answers come only from your own approved administrative content - your billing FAQ, your scheduling policies, your portal help documentation. Not general internet knowledge, not medical reference material the vendor pre-loaded.
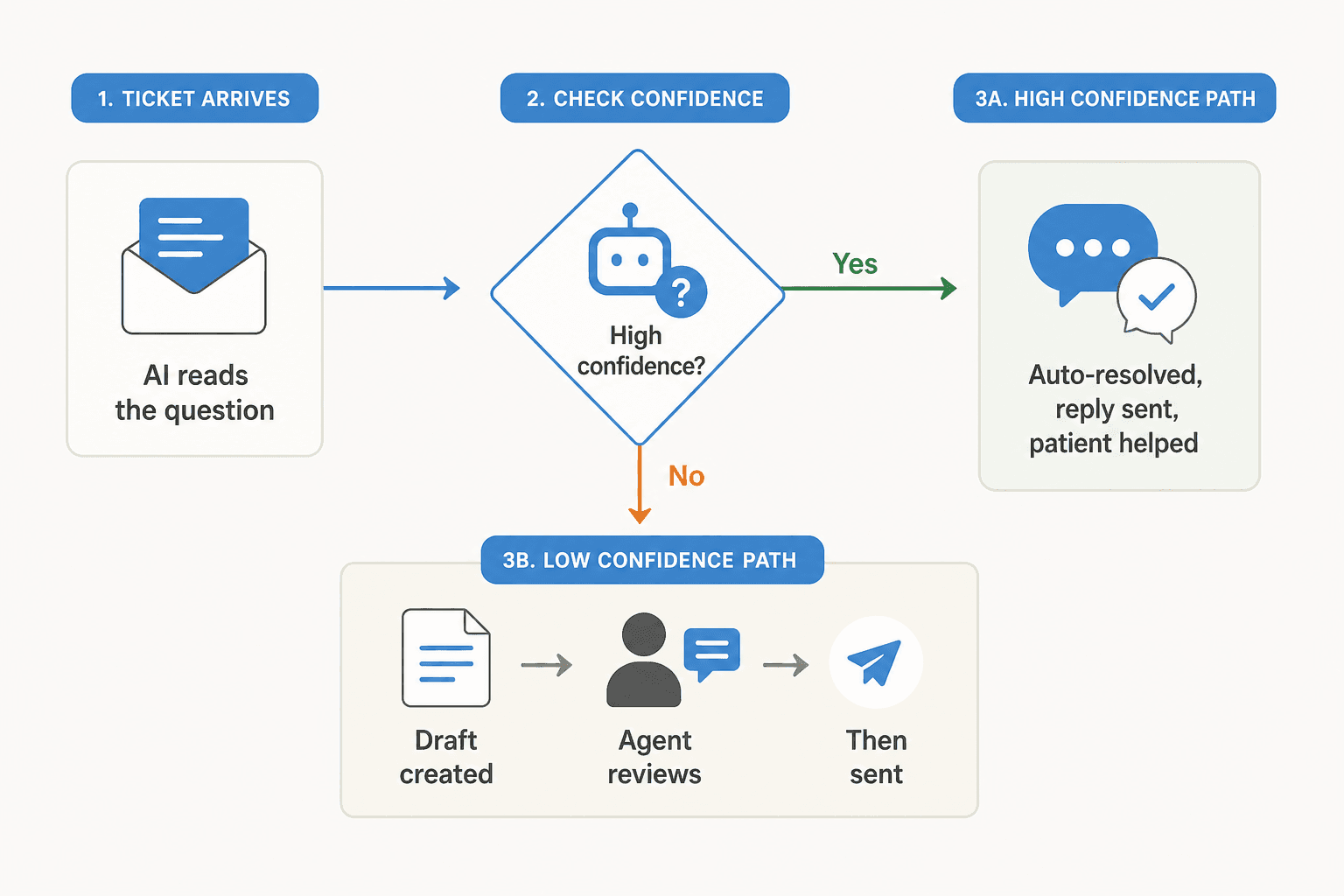
- Routes on confidence. Low-confidence answers become draft replies that an agent reviews before sending. High-confidence administrative answers (office hours, copay lookup, refill status) can send automatically. The threshold between those two is configurable and auditable.
- Never guesses on clinical questions. The scope restriction is architectural, not behavioral - the AI shouldn't even try to answer clinical questions, not just try and fail.
The intake flow above is a clean example: the AI confirms the appointment, the patient confirms back, then the system sends a pre-visit checklist. Every interaction is bounded by administrative content. No step requires clinical judgment. This is what scope restriction looks like in practice.
How to deploy without hitting the standard failure modes
The biggest deployment mistake I see is going live without first seeing what the AI actually does on your tickets. In healthcare that's not an option - you need to know before a patient does.
Here's the deployment sequence that works:
Start with simulation. Before connecting a live queue, run the AI against your historical tickets. Look specifically for: clinical-adjacent questions it tries to answer (billing queries with symptoms mentioned, scheduling requests with condition context), any response where it ventures into clinical interpretation, and the distribution of confidence scores across your actual ticket types. eesel's simulation mode runs against your real ticket history - you see what gets answered, what gets drafted, what gets deflected, and what might need guardrails before the AI meets a real patient. This is the same approach that lets teams improve their AI ticket resolution rate before they expose it to real volume.
Begin in draft/copilot mode, not autonomous. The agent drafts replies for every ticket; a human approves and sends. This gives your team visibility into what the AI is producing across all ticket types before you trust any category to run on its own. Most healthcare teams stay in this mode for 2-4 weeks on a new category before granting autonomy. The key number to watch: what percentage of drafts are you sending as-is vs. editing? Drafts being sent unchanged across a category mean the AI has earned autonomy there. Drafts being heavily rewritten signal the knowledge base needs more work.
Scope the knowledge base deliberately. Connect your billing FAQ, your scheduling policies, your portal help documentation, your insurance and coverage guides. Don't connect your clinical protocols, your provider notes, your EHR content, or anything patients haven't consented to have AI use in responses. This is the architectural guard that prevents clinical scope creep - the AI can't answer from material it hasn't been given.
Set clear escalation triggers. Beyond the confidence threshold, you want hard-coded escalation for specific categories: anything mentioning symptoms, any question about medication, any mention of an emergency. These route straight to a human regardless of confidence score.
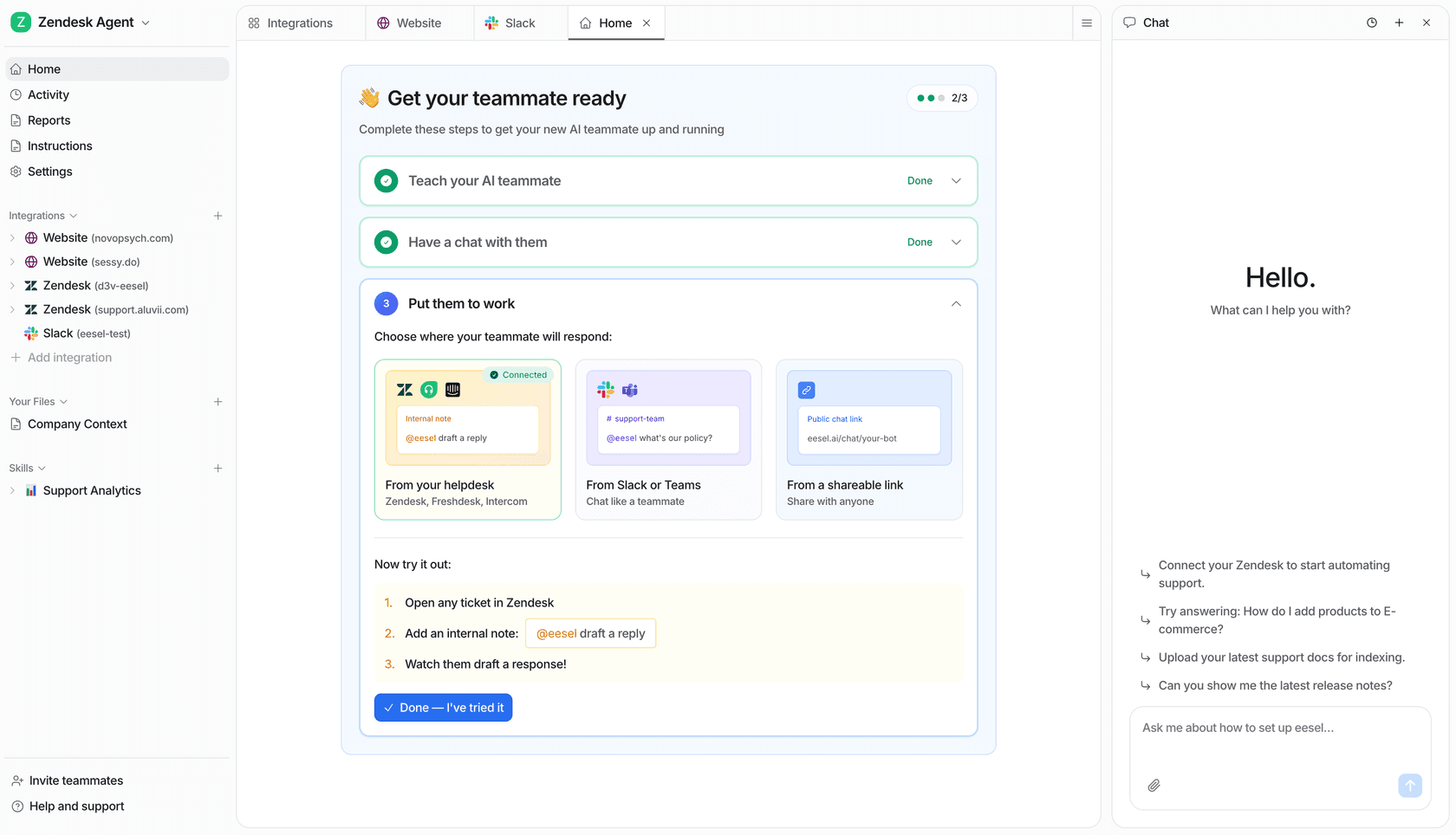
Here's what the eesel agent looks like working on a real support queue - learning from your tickets, drafting replies in the existing workflow, and routing on confidence:
The Gridwise team reported 73% of tier-1 requests resolved in the first month, after results within a 7-day trial. For the full story on what those AI deflection rates look like across different industries and ticket types, the deflection guide has the breakdown. That's a gig-economy app, not healthcare - but the principle transfers. The questions a healthcare support team fields that are analogous to "how do I withdraw my earnings" are the same kind of high-volume, low-variance administrative questions that resolve cleanly once the AI has the right knowledge. In healthcare, those are the appointment and billing queries that make up the majority of most contact centers' volume.
Try eesel
I work at eesel, so this is a transparent recommendation: if you're running a healthcare support team and want to automate the administrative side without building a second compliance infrastructure, eesel is worth looking at.
The relevant facts for healthcare: HIPAA and BAA are on the Enterprise plan. PII redaction strips PHI at ingestion before it reaches any AI provider. Your data never trains any model. The agent runs in draft mode first so you see what it produces before it sends anything autonomously. Simulation mode lets you validate coverage against your actual historical tickets. And it sits on top of whichever helpdesk you already run - Zendesk, Freshdesk, HubSpot, Front - so you're not migrating anything.
The compliance disclosure you'd expect me to give: SOC 2 Type II is in progress, not yet certified. If your procurement team treats the certificate as a hard gate today, say that up front. For a broader look at where AI customer service tools sit on the compliance spectrum - from free tiers that offer nothing to enterprise platforms that cover the full stack - the roundup covers it.
Try eesel - $50 in free usage, no credit card required. The trial is enough to run simulation against your own tickets and see the coverage before you commit to anything.
Frequently Asked Questions
What is AI customer service for healthcare?
Is AI customer service HIPAA compliant?
What ticket types can AI handle in healthcare?
How do I stop an AI support agent from giving clinical advice?
How much does AI customer service for healthcare cost?
What helpdesks does AI customer service for healthcare work with?
What is the biggest mistake healthcare organizations make with AI support?

Article by
Riellvriany Indriawan
Riell is a designer and writer at eesel AI with about two years of experience researching CX platforms, AI chatbots, and helpdesk software. She combines her design background with a sharp eye for how these tools actually look and feel in practice — making her comparisons unusually visual and user-focused.